“Everyone who is seriously involved in the pursuit of science becomes convinced that some spirit is manifest in the laws of the universe, one that is vastly superior to that of man.” – Albert Einstein
It’s a medical miracle, discussed in the video above.
It boils down to this…
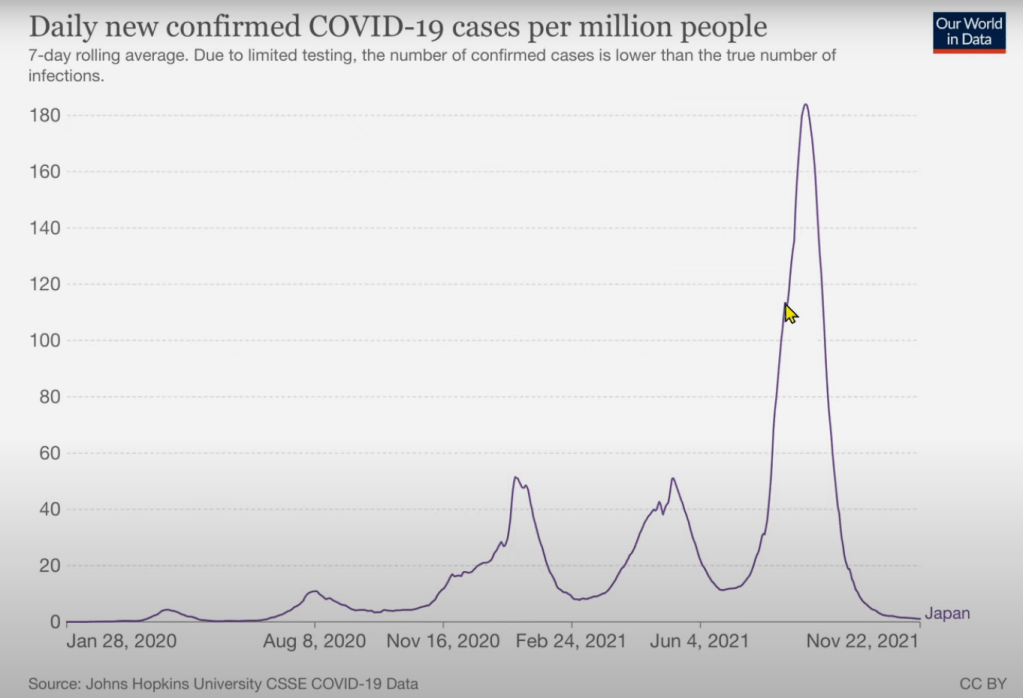
Twelve days after the drug Ivermectin was “OK’d for use” in Japan by Dr. Haruo Ozaki, Chairman of the Tokyo Medical Association, Japan’s sharp spike in COVID-19 cases began a striking decline toward zero as seen in the graph below. The blue arrow points out the day when Doctor Ozaki approved Ivermectin’s use against COVID-19.
For a broader time perspective, here’s that same peak (below on the right). Dr. Ozaki made his announcement at the tip of the yellow pointer.
Note that Ivermectin was not made the “official COVID treatment” in Japan, it was rather OK’d for prescriptive use against COVID for the first time by an official, Dr. Ozaki. Google seems to hide the truth here by deliberately confusing terms and burying all searchers in layers of articles “debunking” the strawman claim that Japan has made Ivermectin their “official COVID treatment.”
Don’t fall for Google’s banana-in-the-tailpipe trick this time.
A cheap and effective COVID drug is the nightmare of major drug companies now. The pandemic has become their cash cow, hence their puppet media suppresses Ivermectin, allowing them time to milk the pandemic at the public’s expense. Sad, but pretty obviously happening.
With a straight face, Doctor John Campbell (a nurse, if I remember right) calls this temporal association “a strange coincidence” in his video and presents a few weak alternative explanations, one of which is not as weak as the others.
I sense Campbell must protect his video from the censors by using the term “strange coincidence” rather than the more appropriate phrase: “a probable cause-and-effect relationship.”
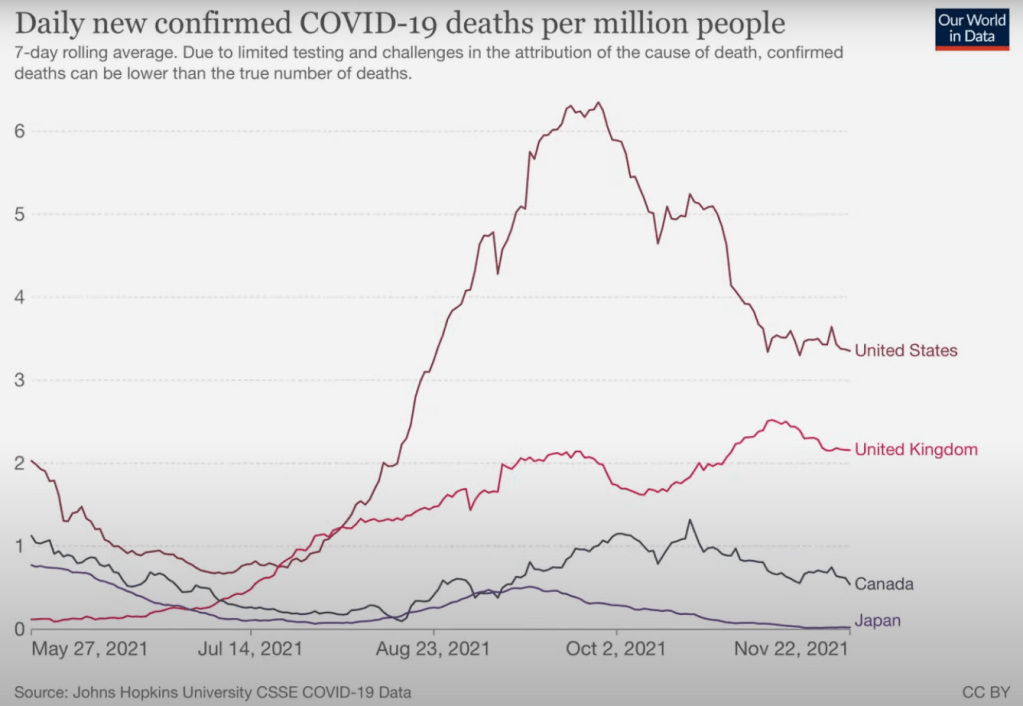
Here’s a current look at the COVID death rates in Japan compared to a few other countries:
The video goes on to offer some alternative explanations for the so-called “coincidence.” One idea not mentioned is the possibility that Ivermectin might somehow be responsible for the mutation discussed that destroys the error-correcting functions of the virus, rendering it impotent. It’s probably a weak idea because Ivermectin most likely has no mutagenic capacity, but who knows? Maybe for this virus it does.
As I’ve said before, the zombie-woke media’s suppression of Ivermectin is idiotic. Someone in power in the US needs to wake up and support the use of this drug. There is growing evidence supporting its effectiveness and an established long track record of its safety within the human population. (No, it’s not “a horse drug” as CNN’s Dr. Gupta had to admit to Joe Rogan. Try finding that video on Google.)
Unfortunately, the brief and increasingly questioned safety record of mRNA vaccines doesn’t compare to that of Ivermectin.
So here’s a perfectly safe, cheap drug that, as best we can tell now, appears to have abruptly stopped the worst peak of COVID-19 in Japan. Shouldn’t we encourage its use in the USA while our universities study its effectiveness? What’s the downside here?
Back in the early 1980’s when I was in pathology residency and HIV / AIDS had begun to burst upon the scene of Western medicine, one of my mentors told me essentially, “This is the first time we face a politically protected disease. There will be many deaths because we didn’t confront this contagion the way we normally would.”
Today it’s hard to imagine that for most gay people back then, their professional careers and social lives would almost certainly be destroyed if they “came out of the closet.”
People of compassion knew this and did everything they could to prevent such cruelty. With the best of intentions they turned a deadly contagious disease into a political affair to protect the gay populations’ valuable privacy.
The medical system decided against using tried-and-true public health measures to protect everyone. Instead they chose to keep the infected victims’ identities secret, to not trace their contacts, and to forget about quarantining the infected individuals.
Traditional public health measures, though logical, seemed cruel and insensitive to many at the time. “Only a hard-nosed conservative homophobe would be so callous and mean-spirited.”
Protected by political emotion, HIV/AIDS spread throughout the world killing millions and millions who might have been spared if the medical community had remained objective and refused to turn an infectious disease into a political issue.
Today the medical community has learned nothing from their tragic emotional response to the HIV epidemic. Again our medical system (in the US) has allowed political emotion to guide them, probably from compassion for the many as yet unvaccinated older adults who are, as far as we know now, statistically much more likely to suffer prolonged illness or death from COVID-19 than from the known side effects of the vaccines.
Sure, this time we underwent extensive public health measures including isolation, politically-motivated mask mandates, and whatnot, but the politically protected disease is now an “uncommon” complication of the vaccine(s).
Since political thinking is black-and-white by nature and has again come to dominate the medical conversation, the vaccines’ negative side effects will not be brought before the public. In politics it always seems better to sweep unwanted things under the rug for the greater political good.
And I almost sort of get it. I personally hesitate to bring vaccine problems to anyone’s attention because:
1. I strongly suspect that the long-term negative effects of the vaccines will be much milder than the overall damage done by COVID-19 itself, after all the facts are known, which won’t be for decades.
2. I share the human tendency for “all-or-none” thinking, so I know that when someone reveals an important flaw in something that’s otherwise quite helpful, regular people like me may view the helpful thing as totally unhelpful. This is an example of using political neurons (rather than our few objective neurons) in allowing the perfect to become the enemy of the good, as for example when our academics’ ideal Bolshevik utopia casts a dark shadow over humanity’s imperfect democracies, and they act to eliminate democracy through the indoctrination of children. Rookie mistake, but so very human.
3. Since the possibility of long-term catastrophically negative side effects of the COVID vaccines cannot be completely ruled out for several decades, I may be sadly mistaken in my assumption that the goodness of COVID vaccines will outweigh all negatives in the final analysis. I’ve made an optimistic but quite reasonable decision in taking the COVID vaccine, specifically at my age (66 now).
But as I say, I’m often wrong about important things, so think for yourself about all sides of this discussion, please, as you consider the “uncommon” but significantly negative early COVID vaccine reactions… exactly how “uncommon,” I don’t know.
But I do know these reactions should be recognized and treated appropriately by the healthcare community.
Unless it’s been taken down by our medically uneducated but well-woke overlords at YouTube, here’s a fascinating (anecdotal) interview of a healthy young athlete who became chronically ill after a second injection of a COVID vaccine that appears to have likely reached his venous circulation directly upon injection…
In summary:
1. The vaccine reaction symptoms, we are told, include postural hypotension, tachycardia, chest pain, weakness, exhaustion after mental or physical exertion, joint pain in areas of old injuries, headache, at least one apparent case of blindness in a young girl, and a number of suicides.
2. Some of these symptoms can last up to 18 months, as far as we now know.
3. The reaction may likely be caused by accidental injection of the vaccine fluid into the (currently ignored) medium-caliber blood vessels that exist somewhat randomly scattered throughout skeletal muscle. (Many MD’s have not cut through a piece of human skeletal muscle since anatomy lab in the first year of med school and have no doubt forgotten, if they ever noticed, the presence of numerous veins and some small arteries within skeletal muscle. These blood vessels have a caliber greater than that of a needle, so injecting directly into them is a physical possibility that would be expected to occur randomly during vaccinations. As a pathologist (retired), I have routinely seen these vessels in the gross room and under the microscope. Someone should do a quantitative study to characterize them in a broad and diverse human population. These small to medium-sized veins and arteries are especially prominent, it seems to me, in the arms of young athletes whose vessels appear to have increased in caliber after years of resistance training.)
4. Healthcare workers need to ALWAYS pull back on the end of the syringe to see if any blood comes back (the “red flash”) from a larger vessel before they inject any intramuscular vaccine or other medication. Please folks, forget the brain-dead dogma that you don’t need this precaution when doing intramuscular vaccine injections! Incidentally, this random, accidental intravenous injection pathway could possibly account for many of the “rare” negative side effects of any other intramuscular vaccines, not merely the COVID vaccines. Think about this, healthcare professional, without listening to your political neurons for once.
5. These vaccine-associated symptoms appear to be lessened by black seed oil, Ivermectin (at least temporarily), and several other over-the-counter items as mentioned in the video above.
6. This vaccine reaction is officially recognized and treated in Singapore, we are told, but still remains largely denied and/or unrecognized in the medical system of the US.
7. In view of the relatively low rate of serious COVID-19 infections in children, it seems reasonable to “allow” parents the right to study the data for themselves and decide whether or not to have their children vaccinated. This seems especially appropriate in the US where addicts (widely considered people with a disease) are free to kill themselves with cigarettes and to donate their life savings to casinos one paycheck at a time.
8. The vaccine reaction is real, but remains politically protected at this time by powerful corporate interests who exert remarkable control over the flow of information in the US.
Here’s a scientific paper (an Indonesian Study that’s not peer-reviewed as yet) showing that people with below normal vitamin D levels have a 10-times greater risk of dying from COVID-19 than people with normal vitamin D levels: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3585561.
The first video below is Dr. John Campbell showing data in which people with darker skin are dying of COVID-19 at a higher rate than people with lighter skin. The stats are shocking, to say the least.
He suggests that since darker skin is less efficient in producing vitamin D3 than lighter skin (because melanin pigment in all races blocks the energy of the sun that drives the chemical conversion of Vitamin D), the higher risk of COVID-19 death for darker-skinned people may be partly due to lower vitamin D3 levels.
He suggests that in the interest of saving the lives of people with darker skin, doctors should check vitamin D levels in COVID-19 patients and “consider” vitamin D3 supplementation for those with low vitamin D levels. Nothing could be more reasonable.
Yet, astonishingly, this doctor has been called a racist for this suggestion. Here’s why:
The malignant and permanently angry religion of Political Correctness dictates that skin color could not possibly affect anyone’s vitamin D3 levels, and low vitamin D3 levels arising from skin color differences could not conceivably reduce a person’s odds of surviving COVID-19. Such unspeakable heresy would suggest that Nature herself is politically incorrect, which would mean the PC worldview itself is fatally flawed. Much better to ignore science and all the non-PC life-saving advantages she offers than to change your worldview.
Below, my favorite research scientist, Rhonda Patrick, PhD, answers various questions about COVID-19, including the Vitamin D question (at position 25:06 on the video). She delves into the relevant peer-reviewed scientific literature.
I should also mention that certain individuals have a condition, probably a genetic SNP (single nucleotide polymorphism), that lowers their vitamin D levels, making it difficult for them to achieve a normal vitamin D level even with D3 supplementation. I know this is real because I have an Asian friend with this trait. So regardless of your skin color, it seems to be entirely worthwhile to have your vitamin D3 level checked, especially now with this lung-attacking virus going around.
Future studies will probably sustain the preliminary data in this post, so be brave and share it with everyone on your email list. You may save someone’s life.